The vast majority of upper limb injuries in swimming are to the shoulder. More than 90%. Then the elbow, then the wrist, and then the finger. Usually wrist injuries are due to overuse or poor technique. Finger injuries occur when hands get smacked against the edge of the pool or hyper-extended in that last desperate lunge to the wall. The trick comes in how to manage these, especially in someone who needs to swim regularly.
It all starts, as it always should and especially with overuse injuries, with a detailed history. If a swimmer is compensating for shoulder pain, extra strain can be felt through the wrist. If a swimmer has had a different injury like a fractured distal radius, then her return to the pool can be compromised not necessarily just by a loss of motion, but more likely due to a loss of forearm strength. A lack of strength can then be exacerbated when swimming equipment like hand paddles are utilised, and wrist stability is compromised. Having said that, if you are sensible, the training aids like fins or paddles can actually help offload an injury. There is almost always a way
to stay in the water.
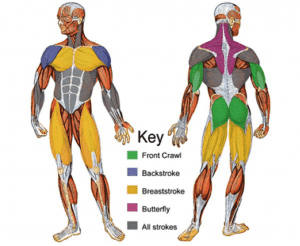 Consider different strokes. It is obvious, or at least should be once you stop and think about it, that breaststroke utilises different muscles to free style. Just have a look at the body shapes of Olympic swimmers. The demands the strokes place on the wrist will change as shoulder position changes. Feathering of the hand through the water will also alter. Use this to your advantage. If one style is inflammatory, can you integrate another so that swimming fitness is maintained throughout recovery? There will be a way.
Consider different strokes. It is obvious, or at least should be once you stop and think about it, that breaststroke utilises different muscles to free style. Just have a look at the body shapes of Olympic swimmers. The demands the strokes place on the wrist will change as shoulder position changes. Feathering of the hand through the water will also alter. Use this to your advantage. If one style is inflammatory, can you integrate another so that swimming fitness is maintained throughout recovery? There will be a way.If you have been told to wear a splint or brace, can you swim with the splint on without posing a risk to how that injury will heal. Paddles can actually help protect a hand fracture, but need to be got used to. I have seen a couple of mallet finger injuries of late caused by hitting the wall too hard. One patient opted not to swim and COVID-19 closing the pool helped with that. The other was a keen open water swimmer. Stupidity personified given it is winter here and the bay sits at around 14 degrees Celsius. However, I'm not judging, really.
The answer here was working out a solid taping protocol both over and under the splint. We also spent some time discussing skin care as the risk of maceration and subsequent skin breakdown was high. Finally, we practiced donning and doffing the splint in the clinic until it could be done confidently without me saying a word.
Water exercise is important for so many reasons. The act of immersion itself can be healing, offering pressure differentials and sensory stimulation, that can reduce oedema, sensitivity, and pain. If you need to get back in the swim, I'm pretty confident that with the right advice, you can.
Look after those fingers,
Hamish











![Stallone, Sylvester [Cliffhanger] photo](https://www.statesidestills.com/prodimages/stallone_sylvester_cliffhanger_58373l.jpg)


























